England's NHS GLP-1 obesity drug rollout described as postcode lottery
Regional access gaps in weight-loss injections like Wegovy and Mounjaro raise concerns as private prescriptions proliferate and rollout timelines stretch into years.
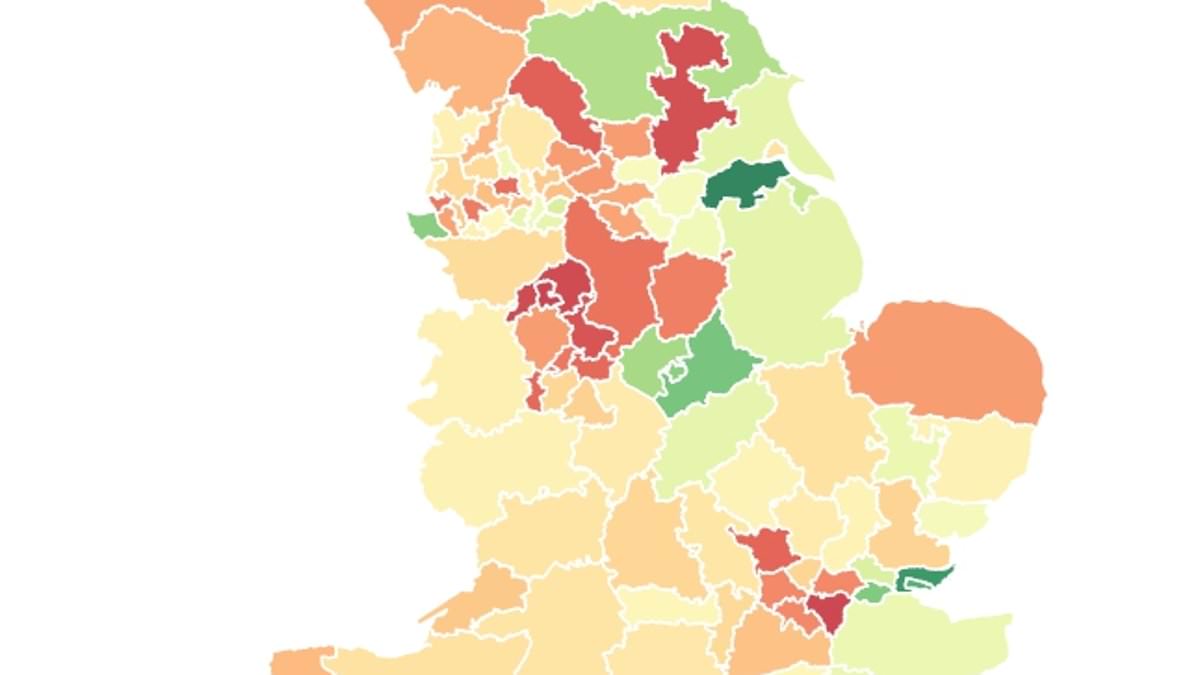
England’s NHS is confronting what health experts describe as a postcode lottery in access to GLP-1 weight-loss injections such as Wegovy and Mounjaro. An analysis of NHS prescribing data paired with obesity population statistics shows wide regional variation in how quickly and what scope the medications are reaching patients deemed eligible under current criteria. Nationwide, about 400,000 GLP-1 prescriptions were issued in June, with most supplies going to private patients outside the NHS framework. Analysts say the result is a two-tier dynamic: some areas are rolling out the drugs more aggressively, while others lack sufficient specialist obesity services to prescribe them through the NHS.
In North Lincolnshire, NHS figures for June show there were 2,445 prescriptions for GLP-1 injections — the umbrella term for the hunger-fighting drugs, which are typically taken weekly or daily. That translated to roughly 1,250 prescriptions per 10,000 obese adults. By contrast, in North Tyneside there were just 265 prescriptions per 10,000 obese adults — a rate the Daily Mail analysis highlighted as part of a broader pattern in which access to the drugs varies dramatically by region. The price tag for NHS access remains a hurdle: the drugs are estimated to cost around £3,000 a year per patient under the current rollout plan, a cost that has prompted caution about expanding access rapidly.
[Image: https://i.dailymail.co.uk/1s/2025/09/18/15/102254071-0-image-m-64_1758206411670.jpg]
Across the country, roughly 400,000 GLP-1 prescriptions were issued in June, with the majority for tirzepatide (Mounjaro) and semaglutide (Wegovy). Other GLP-1 medicines, such as exenatide, dulaglutide and lixisenatide, were dispensed at lower rates. The NHS data do not distinguish whether a prescription was for weight loss or for type 2 diabetes, since the figures cover generic drugs rather than branded versions. NICE guidelines permit Mounjaro, Wegovy and Saxenda for weight-loss use, while Ozempic (semaglutide) remains approved primarily for type 2 diabetes at a lower dose.
The uneven rollout comes as private-sector demand surges. Think-tank and industry observers say private prescriptions — not captured in NHS dispensing data — now account for an estimated 90% of GLP-1 use. High-street pharmacists report private treatment costs as high as £200 a month, helping explain why many patients who do not meet NHS criteria seek privately funded alternatives. The discrepancy in access has fed concerns about widening health inequalities, with some patients able to pay for expedited access while others wait on a phased NHS rollout that could stretch over a decade for all 3.4 million eligible individuals.
Health officials have stressed that the phased rollout is designed to guard against overwhelming primary care. A key bottleneck is the availability of Tier 3 weight-management clinics — specialist services that most patients must navigate to obtain NHS prescriptions for GLP-1s. Not all Integrated Care Boards (ICBs) can deliver across the country, and in some regions there are far more eligible patients than available NHS clinics. For example, a recent UK report highlighted that South East London has more than 130,000 people who could benefit, but only about 3,000 available weight-management places. In other areas, such as Castle Point and Rochford in Essex, and parts of Leicestershire and Rutland, the rollout has progressed more swiftly.
The uneven pattern has prompted a chorus of concern from obesity researchers. Professor Nick Finer, a leading obesity expert, called the situation “a postcode lottery,” noting that many areas lack specialist services capable of prescribing these drugs. “There are areas of the country where there is basically no provision of specialist obesity services,” he said. He emphasized that access should be driven by need and that more areas must develop comprehensive obesity services to ensure safe, scalable delivery.
Professor Jason Halford of the World Obesity Federation echoed the point, acknowledging the short-term cost of these therapies but suggesting that costs should decline as more agents come to market and prices come down. He argued the health system should prepare to scale these treatments, not merely ration them, given their potential to reduce obesity-related mortality from heart disease and cancer.
The private market’s expansion has prompted policymakers to warn of new inequality risks. The Tony Blair Institute for Global Change warned in a May report that the rapid growth of the weight-loss drug sector, combined with a slow NHS rollout, risks creating a two-tier system that compounds health disparities. It cautioned that online pharmacies may fail to serve certain groups, including those with learning disabilities or severe mental illness, who require more tailored support.
Despite the concerns, industry dynamics are shifting as manufacturers anticipate broader competition and price reductions. Novo Nordisk, the maker of Wegovy and Ozempic, has signaled price adjustments as patents expire in some markets and new competitors come online. The NHS is typically able to negotiate favorable prices through bulk purchasing, which some experts believe will help bring costs down over time. As more GLP-1 therapies reach the market, researchers say the scale of rollout could expand, with careful planning to ensure safety and continuity of care across diverse patient groups.
Clinicians emphasize that GLP-1 therapies are not a universal solution for all patients and stress the need to preserve access to other weight-management services. Kamila Hawthorne, chair of the Royal College of General Practitioners, said that while the drugs offer potential benefits for some patients, they should not displace other weight-management strategies. She noted the importance of prevention and a holistic approach that integrates lifestyle support with pharmacotherapy where appropriate, and she urged that the phased NHS rollout be accompanied by training and resources to prevent overburdening primary care.
Public health officials say the goal remains to provide equitable access as part of a broader strategy to tackle obesity. The Department of Health and Social Care has argued that the NHS is testing new ways to deliver these medications to those with the greatest need, while rolling out additional lifestyle support services online and in clinics. In March 2025, the NHS provided funding to local ICBs to support patient care as part of a broader push to extend access in line with NICE guidance and to align with the 10 Year Health Plan’s emphasis on prevention and treatment integration. The department stressed that options beyond NHS prescribing, including digital weight-management programs, are being promoted to ensure patients receive comprehensive care.
Obesity remains a pressing public health issue in the UK. Recent analyses indicate that rising obesity rates have contributed to a decline in life expectancy in England, with the average person living several months less than a decade ago. When combined with the NHS’s budget pressures, the demand for effective, scalable solutions grows more urgent. The government has repeatedly stated that obesity-related costs to the NHS run into billions annually and that reducing obesity is a central aim of policy going forward. As the NHS expands the availability of GLP-1 therapies, officials will be watching for signs that access is becoming more uniform, that waiting times for qualifying patients shorten, and that private use does not outpace NHS provision in a way that exacerbates health inequities. Meanwhile, clinicians will continue to monitor safety, efficacy, and long-term outcomes to ensure that patients receive appropriate care tailored to their medical needs.