Inside Texas's arbovirus lab: a front line against rising mosquito-borne threats
State surveillance in Austin helps detect West Nile, dengue and other vector-borne diseases even as national capacity and funding shrink.
A small laboratory at the Texas State Department of Health Services in Austin is one of the country’s more active early-warning posts for mosquito-borne disease, sorting and testing insects that can carry viruses and parasites that sicken people across the United States.
Scientists at the Arbovirus-Entomology Laboratory conduct weekly mosquito collection analyses, track species and population levels, and run molecular tests for pathogens. The state spends roughly $755,000 a year on its arbovirus surveillance program and employs seven molecular biologists; the program has operated in some form since 1954. "Texas and Florida are the most vulnerable," said Bethany Bolling, manager of the zoonotic virology group at the Texas health department. "A lot of times, we’re the ones that see the first human cases of emerging diseases because of our climate, the vectors that we have, and the population levels."
The lab’s work is part of a broader, uneven system for detecting vector-borne disease in the United States. Federal and state officials say infections spread by animals have more than doubled over the past 20 years, and recent years have seen an uptick in locally acquired cases of diseases that many Americans consider tropical or foreign. West Nile virus was detected this year in 37 states and has caused at least one death; the Centers for Disease Control and Prevention has tallied at least 500 cases nationwide to date. A dengue outbreak that began last year in Puerto Rico and the U.S. Virgin Islands has coincided with locally acquired cases in Texas, California and Florida since 2024. Chikungunya has been detected in at least 60 travelers to the United States this year, though no confirmed local transmission has been reported, and in 2023 the U.S. recorded its first locally acquired malaria cases in two decades in Florida and Texas.
Officials say gaps in surveillance and shrinking resources make it difficult to know the full extent of transmission. "Only about 20 percent of Texas counties do active surveillance," Bolling said, noting that most counties lack the traps, staff and shipping budgets needed to submit samples to the state lab. Local programs that do operate often center around larger metropolitan areas where there are more people and more public health funding. As a result, many outbreaks begin in rural or lower-income areas and are recognized only after people become ill.
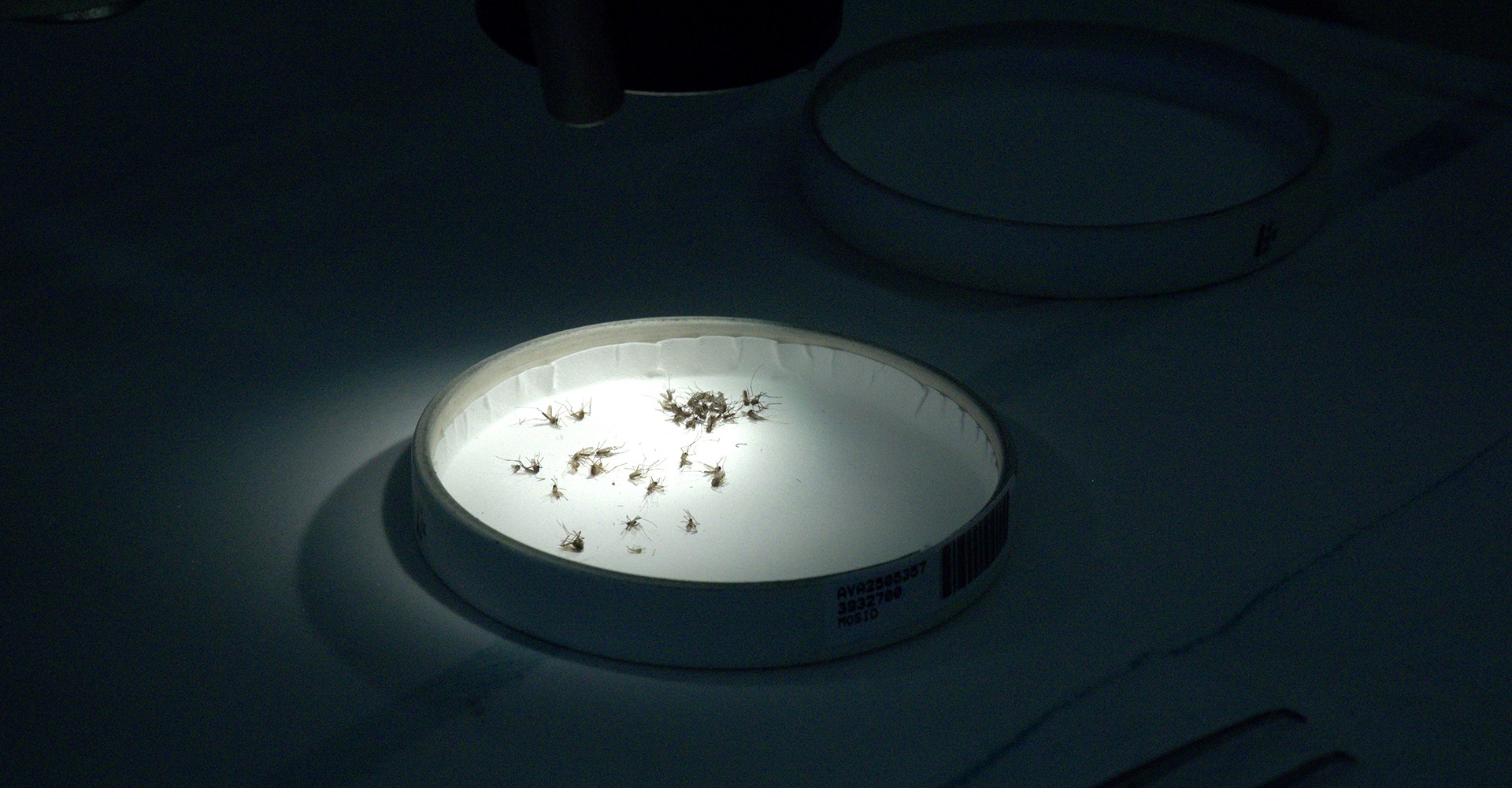
The laboratory space in Austin includes air-pressure–controlled rooms, fume hoods, microscopes and PCR machines. Staff thaw frozen mosquito collections and separate specimens by species to build a picture of which vectors and pathogens are present and where. Identifying the correct species and pathogen informs decisions about targeted control measures; indiscriminate spraying can be costly, ineffective if resistance has developed, and damaging to beneficial insects and ecosystems.

The techniques used to detect pathogens vary in complexity. Polymerase chain reaction, or PCR, can identify known genetic sequences quickly, but it requires prior knowledge of what to test for. Discovering previously unknown viruses requires cell culture assays, in which cells are exposed to mosquito extracts to see if any infectious agents grow — a time-consuming and expensive process that only a small number of U.S. labs are equipped to perform. The Austin lab has temporarily paused some of that work because of staffing shortfalls. "We’re short-staffed a couple of people right now, so we had to put that on hold," Bolling said.
Public-health experts say capacity constraints are not just a Texas problem. The CDC’s ArboNET system is designed as a passive national surveillance network that relies on clinicians to diagnose and report arboviral infections, a process that undercounts cases. The CDC has also established regional training centers and has noted patterns that can signal higher risk — shorter winters, earlier springs and more rainfall are among environmental triggers associated with outbreaks — but translating warnings into local action depends on money, personnel and public buy-in.
Training and workforce development are recurring bottlenecks. Entomologists and public-health insect specialists have traditionally been a small field, and career paths are uneven. To address that gap, educators and researchers have run intensive workshops for health department staff on trap placement, tick and mosquito identification, and field safety. "Vector biology surveillance and management training is more necessary now for public health," said Erika Machtinger, an associate professor of entomology who has helped organize such courses. Advocates emphasize a "one health" approach that connects environmental stewardship, urban planning and public health interventions to reduce transmission risk.
At the same time, federal funding and staffing changes have constrained capacity. Public-health agencies at the state and local level face competing budgetary demands, and some researchers and health officials point to cuts at federal agencies that have reduced the workforce and hampered research into the effects of climate change on disease spread. Public confidence in vaccination and in public-health guidance also affects the tools available to limit outbreaks; a limited number of vaccines exist for vector-borne diseases in U.S. populations, and several more candidates were in development.
Texas's surveillance program illustrates both the promise and the limits of current efforts. The state’s weekly collections and species monitoring can provide early detection that helps protect neighboring states, but the program depends on local partners to trap and ship mosquitoes and on a relatively small team in Austin to analyze samples. Some counties operate their own control measures — Brownsville, for example, maintains in-house trapping, monitoring and spraying — but many do not.
Containment and mitigation strategies include reducing standing water, improving housing to prevent indoor biting, creating habitats for natural mosquito predators, and using targeted insecticides when appropriate. Researchers also point to biological controls: some mosquito species do not bite humans and prey on larvae, and can be components of integrated pest management strategies.
Public-health officials caution that surveillance alone is not sufficient; it must be paired with predictable funding, workforce training, and community-level prevention efforts. Ben Beard, deputy director of the CDC’s Division of Vector-Borne Diseases, said better forecasting tools are a public-health goal, but that forecasting will require improved data and broader investment.
The Austin laboratory continues to sort, test and store specimens, trying to stay ahead of shifting patterns of temperature, rainfall and human movement that shape where and when mosquitoes transmit disease. For now, the state’s program provides a localized model of how sustained surveillance — even on a relatively modest budget — can detect emerging threats early. Officials say expanding that model would take more money, more trained staff and a national commitment to anticipate rather than merely react to vector-borne disease.
Mosquito-borne infections remain preventable in many cases. Local health officials and entomologists emphasize straightforward measures — removing containers that hold water, applying repellents, using window screens and targeting control efforts based on species and pathogen data — alongside investments in surveillance and workforce training to reduce the chance that the next emerging virus becomes the next emergency.