NHS GLP-1 obesity drugs reveal postcode lottery in England
Analysis shows stark regional gaps in access to weight-loss injections, with private prescriptions filling much of the demand and experts warning of growing inequalities.
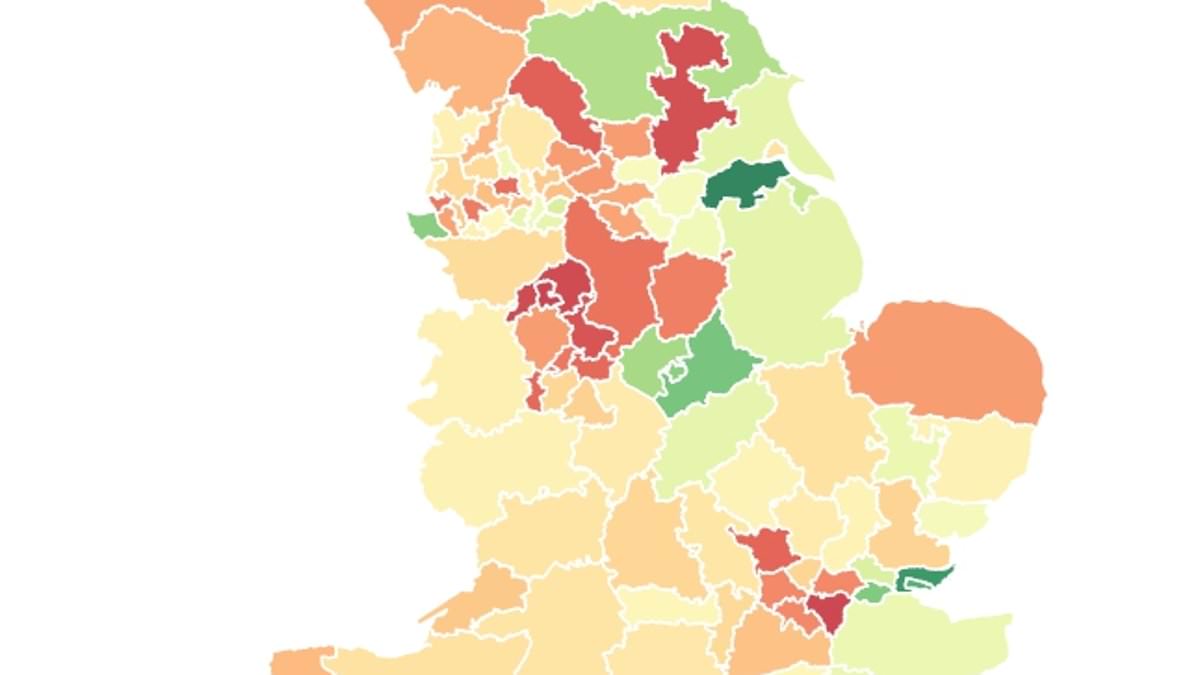
Millions of overweight adults in England cannot access GLP-1 weight-loss injections on the NHS because of what experts are calling a postcode lottery. An analysis of prescribing data and population figures indicates that some areas are far more likely to have patients receiving medications such as tirzepatide (Mounjaro) and semaglutide (Wegovy) than others, even as obesity-related health problems rise. In North Lincolnshire, NHS figures for June show there were 2,445 prescriptions for GLP-1 injections, the umbrella term for these appetite-suppressing drugs, which require weekly or daily use. That equated to about 1,250 prescriptions for every 10,000 obese adults. By contrast, in North Tyneside there were just 265 prescriptions for every 10,000 obese residents.
In recent months, access to these medications has been slowly phased in by NHS spending watchdogs because of the price tag, which the drugs carry at roughly £3,000 a year per patient. Health officials have voiced concerns that GP practices could be overwhelmed if demand surged, potentially delaying the rollout. The program may take up to 12 years to reach all 3.4 million people currently deemed eligible under the existing criteria. As a result, hundreds of thousands of obese patients either go without or pay privately if they can afford it. High street pharmacists can charge as much as £200 a month for private treatment.
The uneven rollout has prompted concerns among experts that a two-tier system is taking shape. Nationwide, about 400,000 GLP-1 prescriptions were issued in June, with the vast majority for tirzepatide and semaglutide. Other GLP-1 types—exenatide, dulaglutide and lixisenatide—also accounted for smaller shares. The pattern of access is shaped in part by the availability of Tier 3 weight-management clinics, which provide the specialist services necessary for NHS prescriptions. Those clinics are concentrated in some regions but lacking in others; in South East London, for example, officials warned that there are roughly 130,000 eligible patients but only enough weight-management places for about 3,000.
Adults seeking NHS access typically must meet criteria that include a BMI threshold (generally 27.5 or higher, depending on ethnicity and the drug) and weight-related health problems. But with many care boards lacking capacity to deliver the necessary services to all eligible people, private prescriptions have become a major channel for access. Industry observers estimate that as much as 90% of GLP-1 prescriptions are now issued privately, a dynamic that underscores the gap between policy and patient need. Some patients have even attempted to circumvent NHS rules by misreporting weight or height to online providers, a problem experts say highlights the pressure on the system.
Professor Nick Finer, a leading obesity researcher, described the situation as a genuine postcode lottery. “To me, it is truly extraordinary that the health service has been so slow to deliver the drugs to people who need them,” he said. He attributed the uneven access to a wide disparity in obesity services across integrated care boards (ICBs), noting that some regions lack specialist obesity services entirely. Professor Finer added that while private prescriptions have filled some gaps, they do not reflect universal NHS access, and the lack of a nationwide, uniform program risks widening health inequalities.
Other experts weighed in on the policy design. Professor Jason Halford of the World Obesity Federation emphasized the short-term cost hurdle but warned that as more treatments come online, prices should fall and rollout could scale up more quickly. Kamila Hawthorne, chair of the Royal College of GPs, cautioned that weight-loss medications are not a “silver bullet.” She stressed the need to maintain a broad approach that includes prevention and other weight-management services so that no single intervention dominates care.
The private market is thriving while the NHS rollout continues. Roughly 1.2 million well-off Britons are reportedly paying privately for these drugs, and analysts at think tanks have warned that the current pace risks creating a two-tier system where wealthier patients gain quicker access. The Tony Blair Institute for Global Change warned in a May report that the rapid growth of the weight-loss drugs market, coupled with a slow NHS rollout, could deepen health inequalities, particularly as obesity remains more prevalent in more deprived communities. Online pharmacies, the report noted, may fail to adequately serve groups such as those with learning disabilities or severe mental illness who require more personalized support.
Pharmaceuticals companies have also signaled shifts in the market. The US-based maker of Mounjaro announced a jump in wholesale price for its highest-dose product starting in September, from about £122 to £330 per month, prompting pharmacies to caution patients about “panic buying.” In the UK context, NHS and NICE guidance continues to define which patients qualify for treatment through the state, with Ozempic (semaglutide) approved for diabetes at a lower dose and Wegovy and Mounjaro approved for weight loss under weight-management criteria. Saxenda (liraglutide) was the first GLP-1 approved for weight loss in 2017, followed by Wegovy in 2023 and Mounjaro in 2024; Ozempic remains diabetes-focused at lower dosage levels, and Victoza is a diabetes-only liraglutide formulation.
In response to the growing demand and inequities, government and NHS officials have defended the phased rollout as a prudent approach to ensure patient safety and system capacity. A Department of Health and Social Care spokesperson said more must be done to make drugs available nationwide and noted that some areas are already testing new delivery models to reach those with the highest need as part of the 10-year health plan. An NHS spokesperson reiterated that weight-loss medications play a vital role for many patients and that the service is developing a holistic set of supports, including a digital weight-management program and other lifestyle resources, to accompany GP prescriptions. The agency said the phased rollout to tirzepatide (Mounjaro) is underway with guidance aligned to NICE recommendations, and funding has been provided to local ICBs to support patient care as of March 2025.
Beyond access, health policy researchers point to the broader burden of obesity on public health. Government assessments have consistently shown obesity costs the NHS billions annually and is a major preventable driver of cancer and other illnesses. An analysis last year estimated that the average obese individual costs the NHS at least £1,000 per year in healthcare costs. Other studies have suggested that obesity-related losses in life expectancy have contributed to a net decline in average English lifespan over the past decade. In this context, experts say the potential of GLP-1 therapies to reduce mortality from heart disease and cancer is substantial, underscoring the importance of a scalable, equitable rollout.
As the NHS continues to expand access, stakeholders emphasize the need for real-time monitoring of service capacity and equity. Dr Nerys Astbury, a diet and obesity researcher at the University of Oxford, noted that the number of people living with obesity is rising and that healthcare systems must prepare to meet growing demand without compromising care quality. The overarching goal remains clear: ensure that the most effective treatments are accessible to those who need them most, regardless of geography, while continuing to invest in prevention and broader obesity-management services.