Thumb Test May Signal Heart Risk, But Not a Diagnosis, Experts Say
Medical professionals caution that the thumb-palm sign is not a diagnostic tool for aneurysms, though it can prompt discussion and targeted screening.
A simple home check known as the thumb test has surfaced as a potential signal of elevated risk for an aortic aneurysm. While some people may find the maneuver informative, clinicians stress that the test is not diagnostic and should not replace formal screening or imaging for aneurysm. The test is described as a quick bedside sign that may reflect joint laxity, which can be associated with certain inherited connective tissue conditions.
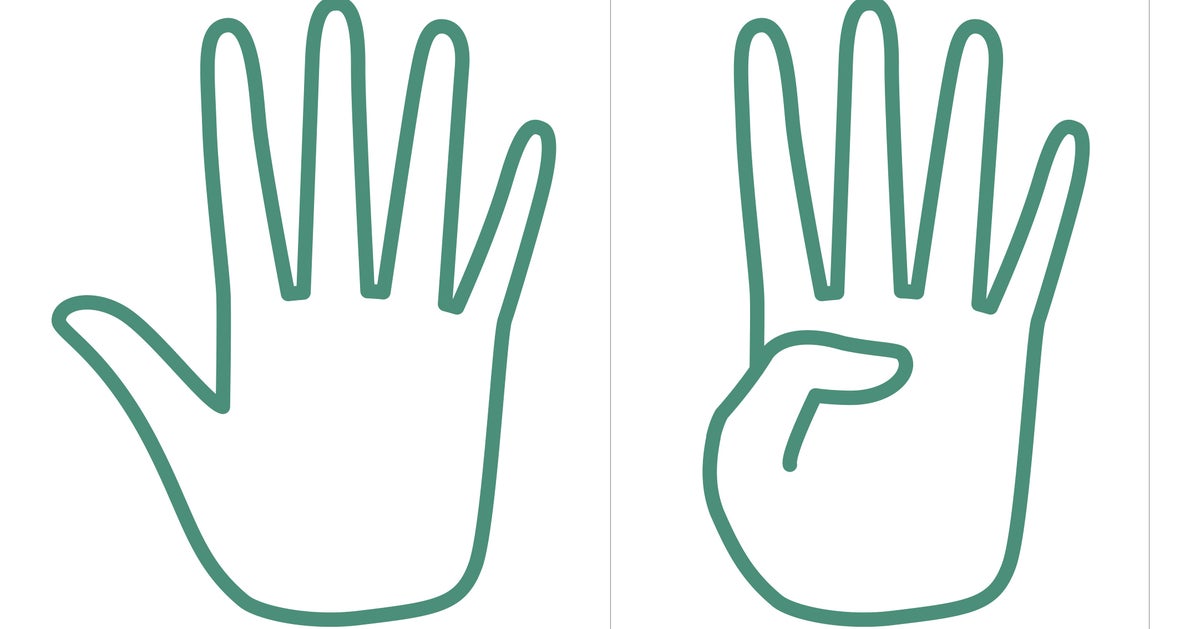
The thumb test involves laying the thumb across a flat palm. If the thumb extends beyond the edge of the palm, it may indicate joint hypermobility and a pattern linked to connective tissue disorders such as Marfan syndrome and Ehlers-Danlos syndrome. These conditions can be associated with a higher risk of aneurysms because blood vessel walls may be weaker. Importantly, a positive sign does not prove that an aneurysm is present and a negative sign does not rule it out. In a 2021 study, people with a positive thumb sign were more likely to have an ascending aortic aneurysm, but most aneurysm patients did not exhibit the thumb-palm sign.
Experts caution that the thumb test should not be used as a screening tool for aneurysm. It is not considered reliable or accurate on its own, and many healthy individuals may show a positive sign. Conversely, many patients with aneurysms may have a normal thumb test. Relying on this sign could delay appropriate screening or surveillance with imaging. Imaging technologies such as echocardiography, CT, or ultrasound remain the gold standard for diagnosing an aneurysm and are recommended based on risk factors and guideline-based protocols.
If you have a positive thumb test, you should discuss the finding with a clinician to determine whether it could point to an underlying connective tissue condition and whether further testing is warranted. A clinician may conduct a full physical examination and order imaging studies if indicated by risk factors or family history. If a positive sign coincides with features suggestive of Marfan syndrome or Ehlers-Danlos, or if there is a family history of aneurysm or dissection, formal evaluation and targeted aortic imaging may be recommended. Otherwise, an isolated positive result in an otherwise healthy person usually does not require urgent action but can be mentioned at a routine visit for context.
Risk factors for an aortic aneurysm extend beyond a positive thumb sign and include age over 65, male sex, smoking, high blood pressure, connective tissue disorders, a family history of aneurysm or dissection, and the presence of a bicuspid aortic valve. These factors help guide decisions about screening and monitoring, as guidelines emphasize imaging when warranted by risk assessments rather than by a single bedside test.
Ultimately, the thumb test can prompt useful conversations about heart and vessel health, but medical decision-making should be guided by evidence-based screening and imaging. Clinicians encourage patients to discuss risk factors with their doctors to determine when screening and monitoring are appropriate. In short, the thumb test may raise awareness of potential issues but should not replace guideline-based evaluation or imaging when assessing aneurysm risk.